



Distal Biceps Rupture
Welcome to Orthosports Question for Physiotherapists February 2024. This month Dr Doron Sher discusses management of distal biceps rupture. If you have a Question that you
Sport after Total Knee Replacement
Welcome to Orthosports Question for Physiotherapists, October 2023. This month Dr Doron Sher discusses return to sport after total knee replacement. REMINDER: Register your place for the Annual Orthopaedic Updates.
High Tibial Osteotomy and Uni Knee Replacement
Welcome to Orthosports Question for Physiotherapists, September 2023. This month Dr Doron Sher discusses the comparison of the High Tibial Osteotomy vs the Unicompartmental Knee Replacement. Register your
Achilles Tendon Ruptures
Welcome to Orthosports Question for Physiotherapists, August 2023. This month Dr John Negrine discusses Achilles Tendon Ruptures. Save the Date: Saturday, 4th November, 2023 Annual Orthopaedic Updates. Live
Lateral extra-articular tenodesis
Welcome to Orthosports Question for Physiotherapists, June 2023. This month Dr Michael Goldberg discusses lateral extra-articular tenodesis and why you would add this procedure to an ACL
Adding a Patch to Rotator Cuff Repairs
Welcome to Orthosports Question for Physiotherapists, May 2023. This month Dr Doron Sher discusses the use of a patch in Rotator Cuff Repairs. Save the Date: Saturday, 4th
Imaging for ACL Injury
Welcome to Orthosports Question for Physiotherapists, October 2022. This month Dr Doron Sher discusses imaging for a suspected ACL injury. Save the Date: Saturday, 12 November, 2022 Annual
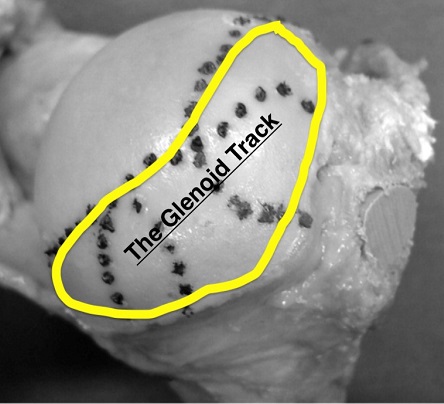
Glenoid Track and Shoulder Instability
Welcome to Orthosports Question for Physiotherapists August, 2022. This month Dr Doron Sher discusses a question on the glenoid track and shoulder instability. Save the Date: Saturday,
OSTEOCHONDRITIS DISSECANS
Welcome to Orthosports Question for Physiotherapists May, 2022. This month Dr Doron Sher discusses a question on treatment options for an OCD Lesion. Save the Date: Saturday,
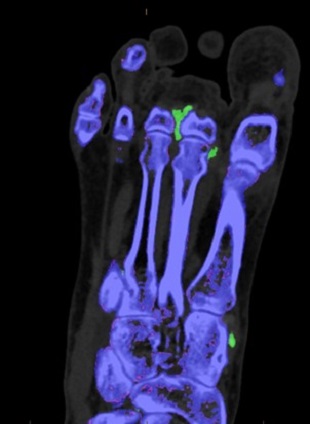
Accessory Bones of the Foot and Ankle
Welcome to Question for Physiotherapists, April, 2022 This month Dr John Negrine discusses accessory bones of the foot and ankle. Please feel free to send your
Hypermobile Lateral Meniscus
Welcome to Question for Physiotherapists, March, 2022 This month Dr Michael Goldberg discusses the Hypermobile Lateral Meniscus. Please feel free to send your questions to

Imaging in Musculoskeletal assessment
Welcome to Question for Physiotherapists, February, 2022 This month Dr Paul Annett discusses Imaging inMusculo-skeletal Assessment. Please feel free to send your questions to education@orthosports.com.au Dr
Shoulder Injury related to vaccine administration
Welcome to Question for Physiotherapists, January, 2022 This month Dr Doron Sher discusses Shoulder Injury related to Vaccine administration. Please feel free to send your questions
Chondral Grafting in the knee
Welcome to Question for Physiotherapists, November 2021. This month Dr Doron Sher discusses Chondral Grafting in the knee.Please feel free to send your questions to education@orthosports.com.au CHONDRAL

Syndesmosis Fixation
Welcome to Question for Physiotherapists, October 2021. This month Dr Todd Gothelf discusses Syndesmosis fixation. Please feel free to send your questions to education@orthosports.com.au QUESTION I

Hip Precautions following Total Hip Replacement
Welcome to Question for Physiotherapists, September 2021. This month Dr Christopher Spelman discusses precautions after a Total Hip Replacement. Please feel free to send your questions
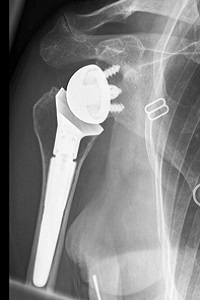
Reverse Shoulder Replacement Rehabilitation
Welcome to Question for Physiotherapists, August 2021. This month Dr Doron Sher discusses rehabilition after a Reverse Shoulder Replacement. Please feel free to send your questions
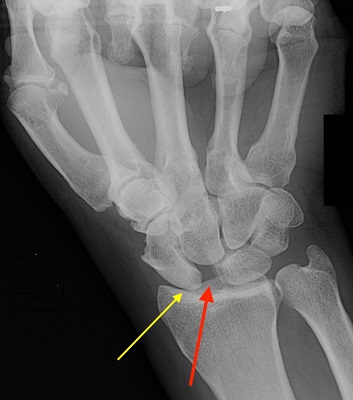
Chronic Scapholunate Ligament Rupture
Welcome to Question for Physios, July 2021. This month Dr Kwan Yeoh discusses the management of Complete Scapholunate Ligament Rupture. Please feel free to send your

Assessing Sports Injury
Welcome to Question for Physiotherapists June 2021. This month Dr Paul Annett presents an article on assessing a patient that presents with potentially more than a

Discoid Lateral Meniscus
Welcome to Question for Physiotherapists May 2021. This month Dr Doron Sher presents an article on a Discoid Lateral Meniscus. Please feel free to send

Cavo-Varus (High Arched) Feet
QUESTION | Why are high arched feet more interesting than flat feet? ANSWER | A 43 year old man presents with numbness on the outer

Surgical Treatment of Unstable Shoulder
QUESTION | | Surgical treatment of the unstable shoulder – How do you decide which patient gets what operation? We know that younger patients and those
Full Thickness Tear of Supraspinatus Tendon
QUESTION | My patient is a 67 year old female who has had pain during overhead activity (catching pain), going on for over 5 years.

Medial Meniscal Root Tears
QUESTION I I have a patient in her 50s who has had a meniscus repair done. I thought that the studies showed no advantage when doing
Wrist Ganglion & Carpal Instability
QUESTION| How Does a Wrist Ganglion relate to Carpal Instability? How is it best treated? ANSWER | A ganglion is a benign synovium-lined cystic collection of

Lumbar Stress Fractures
QUESTIONS | 1. What is rest in treatment of stress fracture? Walking only? Bike? Swim(in non-extended position)? What can you do? Or is it just not

Collateral Ligament Tear
QUESTION | WHEN DOES A COLLATERAL LIGAMENT TEAR OF THE THUMB NEED SURGERY? ANSWER | For the purposes of this question, I’m going to assume
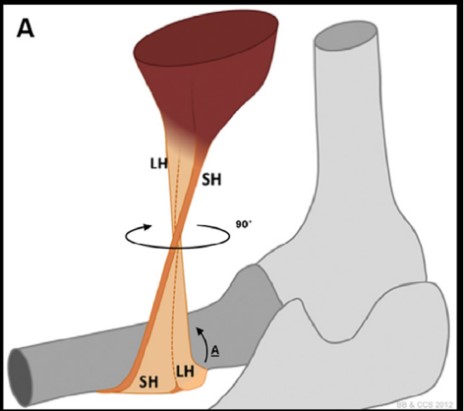
Distal Biceps Rupture
QUESTION | I recently had a patient with a partial distal biceps rupture. Why was he offered surgery without trying non-operative management? ANSWER | Anatomy:

Hallux Rigidus
QUESTION | What are the best options for a 50 year old runner with Hallux Rigidus? ANSWER | A 50 year old runner with hallux